DDH (Hip dysplasia), perthes and all hip and knee conditions
What is developmental dysplasia of the hip (DDH)?
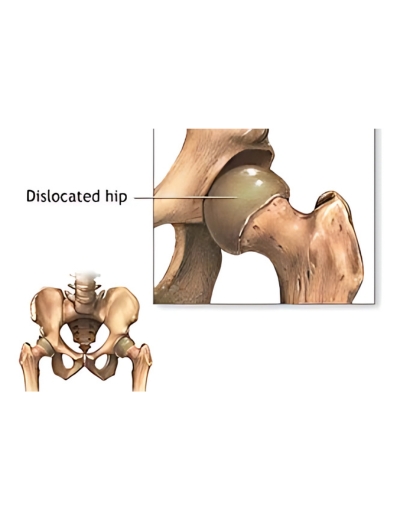
Developmental dysplasia of the hip (DDH or hip dysplasia) is a relatively common condition in the developing hip joint. It occurs once in every 1,000 live births. The hip joint is made up of a ball (femur) and socket (acetabulum) joint. In DDH, this joint may be unstable with the ball slipping in and out of the socket.
In addition, the socket is often shallow which can increase a person’s risk of developing arthritis and joint pain later in life. Hip dysplasia has wide spectrum of severity ranging from a mildly shallow hip socket to a completely dislocated hip.
The greatest incidence of DDH occurs in first-born females with a history of a close relative with the condition and/or history of breech position in utero.


Causes
The exact cause(s) of hip dysplasia are unknown, but it is likely that many factors both environmental and genetic play a role.
One of the environmental influences thought to contribute to hip dysplasia is the baby’s response to the mother’s hormones during pregnancy. A tight uterus that prevents fetal movement or breech position may also cause hip dysplasia. The left hip is involved more frequently than the right due to intrauterine positioning.
Another environmental factor is infant positioning in the first year of life. Cultures that hold infants wrapped around a caregiver such that the hips are held apart generally have lower rates of DDH. In contrast, cultures which typically swaddle or papoose an infant with the hips extended have high rates of hip dysplasia.
Risk factors for DDH
First-born babies are at higher risk since the uterus is small and there is limited room for the baby to move; therefore affecting the development of the hip. Other risk factors may include the following:
- Family history of developmental dysplasia of the hip, or very flexible ligaments
- Position of the baby in the uterus, especially with breech presentations
- Associations with other orthopaedic problems that include metatarsus adductus, clubfoot deformity, congenital conditions, and other syndromes
- Frequent swaddling with the hips out straight (extended)
Symptoms
The symptoms of hip dysplasia are often very subtle during the newborn period. Hip dysplasia is painless during infancy and early childhood though it can cause pain and disability later in life if left untreated. Characteristic findings which raise a suspicion for DDH include:
- The leg that appears shorter on the side of the dislocated hip
- The affected leg not spreading (abducting) as widely as the normal side
- The folds in the skin of the thigh or buttocks may appear uneven
- A “clunk” felt with diaper changes or other positioning of the leg.
If unrecognized until later in life, children with DDH will still typically learn to walk at a normal age. Depending on the severity of hip dysplasia, a child may have a limp or “waddle” with walking or running.
Pain and leg length differences can develop during adolescence. During adulthood, residual shallowness in the hip socket is thought to be the number one cause of arthritis and therefore the most common reason for why an adult may require a hip replacement (artificial joint).
Treatment
Specific treatment for DDH will be determined by your baby’s physician based on:
- Your baby’s gestational age, overall health, and medical history
- The severity of the condition
- Your baby’s tolerance for specific medications, procedures or therapies
- Your opinion or preference
The goal of treatment is to put the femoral head back into the socket of the hip and to deepen the socket so that the hip can develop normally. Treatment options vary for babies and may include:
Pavlik harness
The Pavlik harness is used on babies up to 6 months of age to guide the hip into place, while allowing the legs to move a little. The harness is put on by your baby’s physician and is usually worn full time for several weeks, then part-time for an additional number of weeks.
Your baby is seen frequently during this time so that the harness may be checked for proper fit and to examine the hip. During the course of treatment, ultrasound (or x-ray) will be used to check hip placement and the development of the socket.
Most hips in infants can be successfully treated with the Pavlik harness, but sometimes, they may continue to be partially or completely dislocated.
Abduction bracing
If the hip continues to be partially or completely dislocated, the second line of treatment is an abduction brace, which is more rigid and can be used beyond 6 months of age in older and bigger infants.
These braces generally allow less motion than a Pavlik harness and are therefore more restrictive but can be quite successful for those infants in whom the Pavlik does not work.
Body casting (spica casting)
If the harness and/or brace are not successful, a procedure under anesthesia may be required to put the hip back into place manually, also known as a closed reduction. If successful, a custom molded body cast (called a spica cast) is put on the baby to hold the hip in place. The hip spica cast is usually applied from the chest down to the ankle of the affected side and usually includes part of the opposite leg as well.
The spica cast is worn for approximately three to six months. The cast is changed from time to time to accommodate the baby’s growth and for hygiene reasons. Following casting, a brace and/or physical therapy may be necessary to promote deepening of the hip socket and strengthen the muscles.
Pre-OP & Post-OP Pictures
Post trauma (Exposed bone)
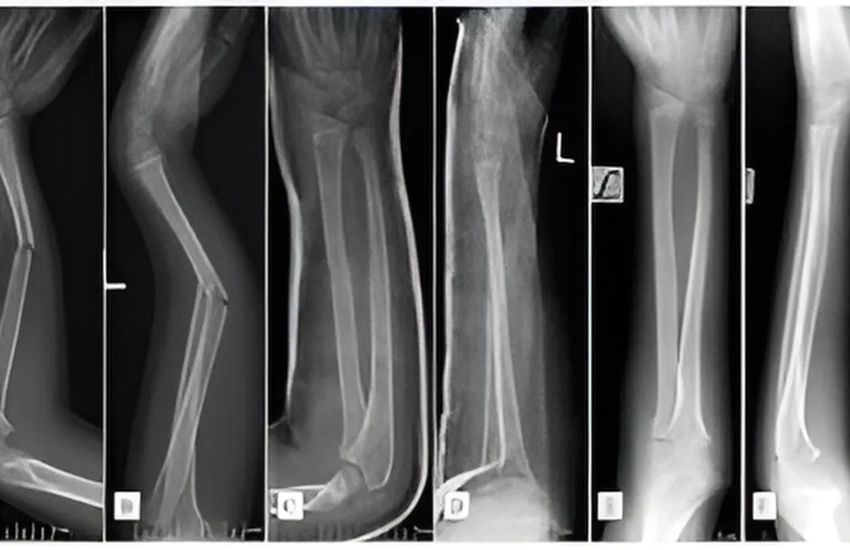
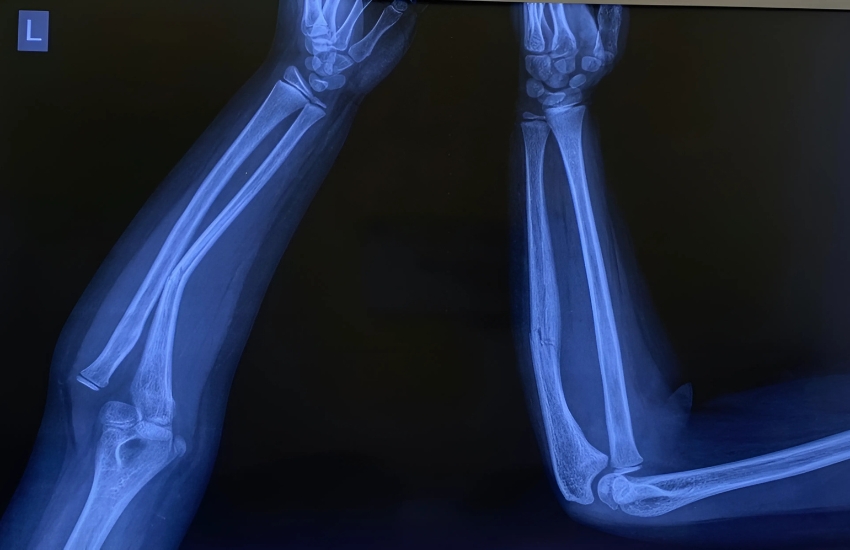
Paediatric forearm Open fracture with exposed bone
Road Traffic Accident with open wound
Road Traffic Accident with Open tibia fracture advised amputation elsewhere saved his leg with multiple surgery
Bone Lengthening
Gradual Bone Lengthening using Orthofix
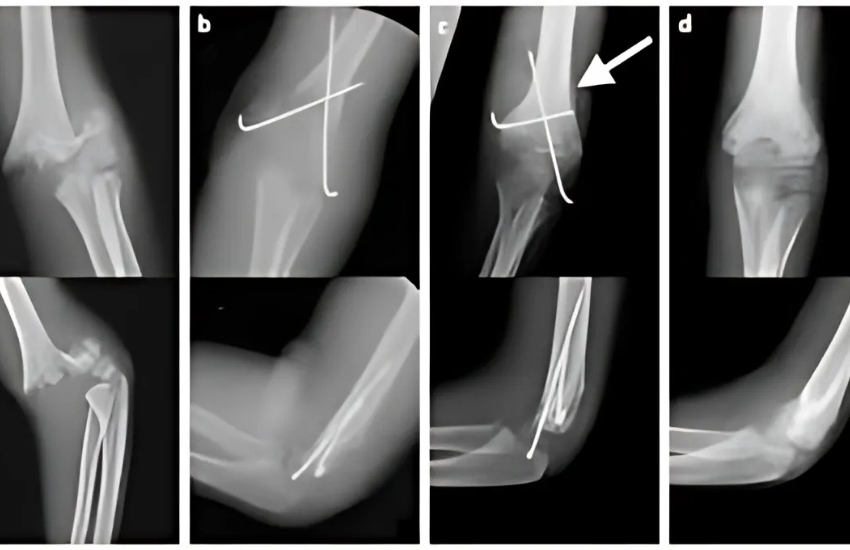
MONTEGGIA FRACTURE DISLOCATION
Monteggia Fracture dislocation treated with plaster without surgery

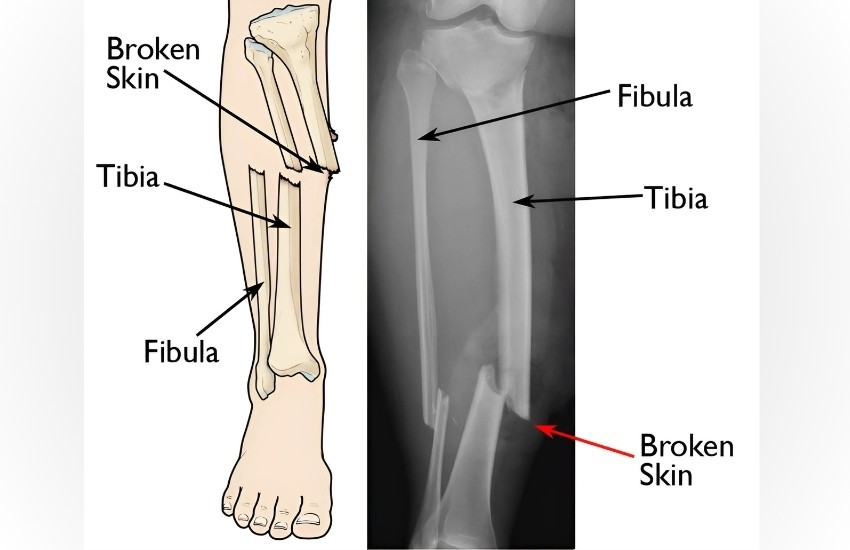
Open Tibia Fracture
Open Tibia Fracture managed with elastic nail and JESS fixator
Bone and soft tissue tumors
Minimally invasive surgery to correct the deformity without cutting the bone with single screw (day care surgery)

Middle Phalanx Fracture
Neglected Middle Phalanx Fracture managed with minimally invasive surgery with mini JESS Fixator

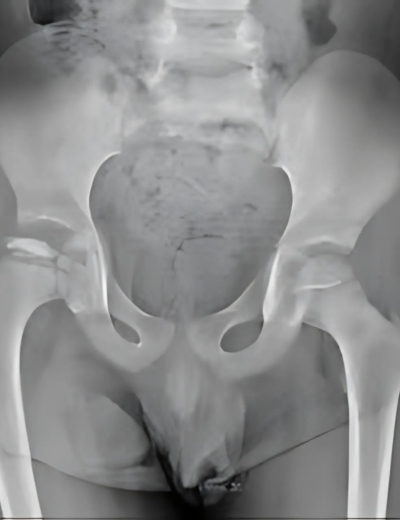
DDH xray
3 years old child with right hip Dysplasia with dislocation underwent open reduction and femoral shortening and varus derotation osteotomy

Hip Joint
4 years old girl with left hip joint subluxation with coxa valga (post septic) underwent left hip Open Reduction and proximal femur varus derotation osteotomy and hip spica
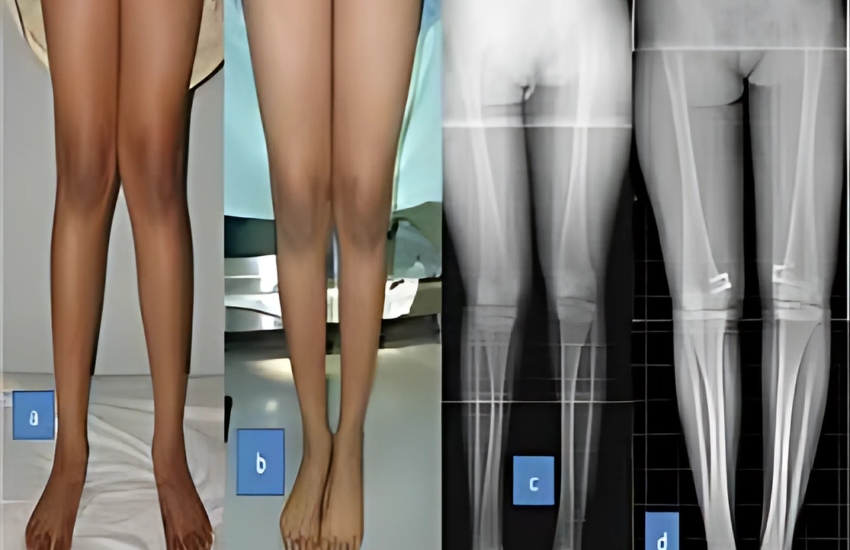
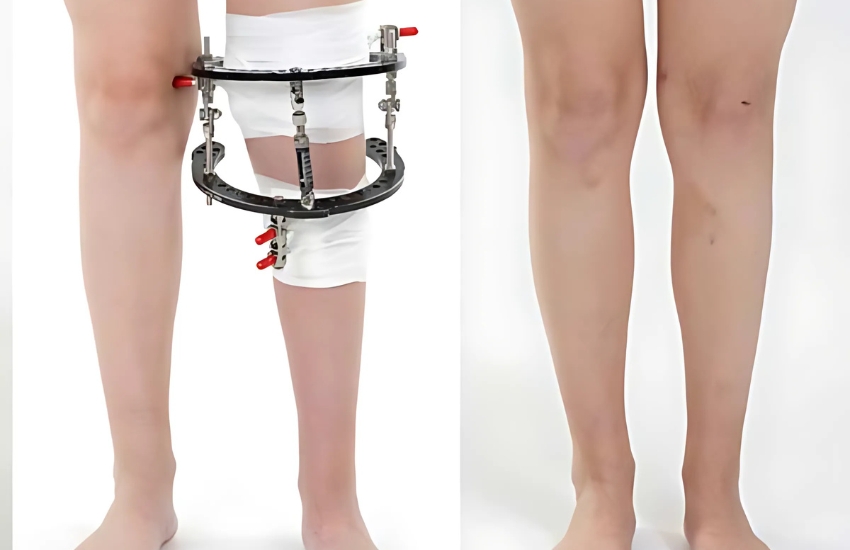
GENU VALGUM PREOP AND POST OP IMAGES
Bilateral genu valgus deformity correction with osteotomy

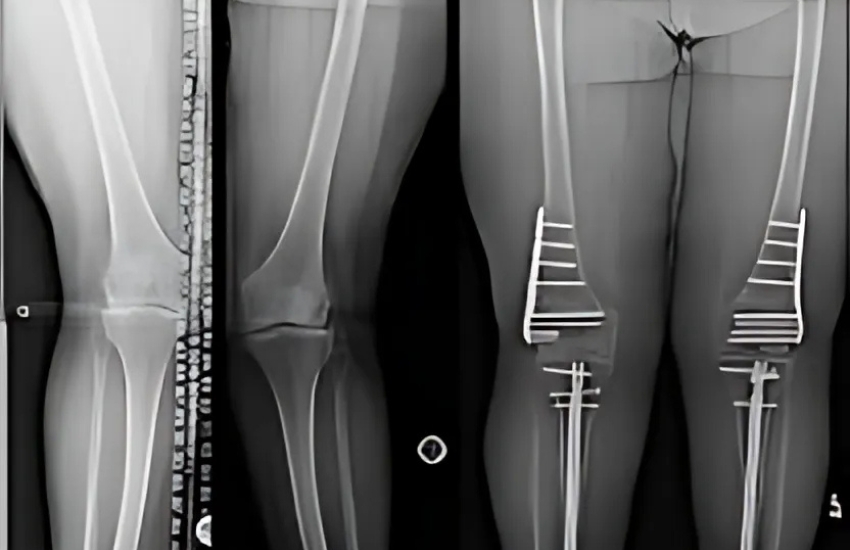
Deformity
knee deformity (blount disease) genu varum left side
Supracondylar Fracture
This is supracondylar fracture in a 5yr old child after slip and fall while playing ( x ray before surgery )

SC Fixation
SC# AP view after reduction and fixation
Road Traffic Accident
AFTER ankle and femur fixation surgery